What Is Heel Pain And The Way To End It
Overview
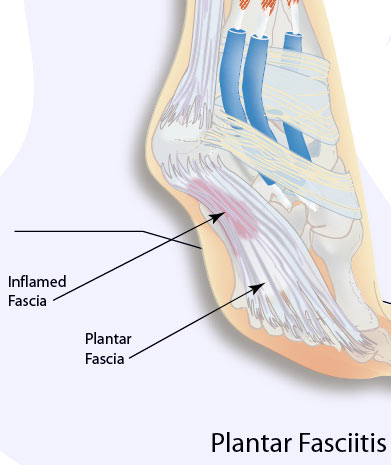
Plantar Fasciitis is the most common condition of heel pain. This condition occurs when the long fibrous plantar fascia ligament along the bottom of the foot develops tears in the tissue resulting in pain and inflammation. The pain of plantar fasciitis is usually located close to where the fascia attaches to the calcaneous, also known as the heel bone. The condition is often misspelled as: plantar fascitis, plantar fasciatis, planters fasciitis, plantar faciatis, and plantar faciaitis. Plantar fasciitis causes the inflammation of the plantar fascia ligament which runs along the bottom of the foot. The plantar fascia ligament is made of fibrous bands of tissue and runs between the heel bone and your toes and stretches with every step. Inflammation develops when tears occur in the tissue. The most common complaint from plantar fasciitis is a burning, stabbing, or aching pain in the heel of the foot. Most sufferers will be able to feel it in the morning because the fascia ligament tightens up during the night while we sleep, causing pain to diminish. However, when we climb out of bed and place pressure on the ligament, it becomes taut and pain is particularly acute. Pain usually decreases as the tissue warms up, but may easily return again after long periods of standing or weight bearing, physical activity, or after getting up after long periods of lethargy or sitting down. In most cases, plantar fasciitis does not require surgery or invasive procedures to stop pain and reverse damage. Conservative treatments are usually all that is required. However, every person's body responds to plantar fasciitis treatment differently and recovery times may vary.
Causes
Currently no single factor has been reliably identified as contributing to the development of plantar fasciitis. The two risk factors with the most support from current research. Decreased ankle dorsiflexion. Increased Body Mass Index (BMI) in non-athletic populations. These factors are related in that both lead to increased strain on the arch, both lead to increased compression on the heel. When dorsiflexion range of motion (ankle flexibility) is lacking, the body compensates by increasing movement of the arch. In this way, decreased ankle dorsiflexion influences pronation and places strain on the underside of the foot. Similarly, having a high BMI causes strain because it places a load on the foot that may be in excess of what the foot can support. As mentioned earlier, overpronation is thought to be a contributing factor, but studies on this have so far produced mixed results. The second way these factors relate to each other is in the way people stand. A lack of ankle flexibility and a high BMI can both cause increased pressure on the heel in standing. Keeping weight on the heels causes compression under the heel. But it also means the muscles and ligaments in the arch are not being used to balance your body weight. Lack of use, I suspect, is a greater danger than overuse. Looking beyond these potential contributors to heel pain though, there is one major factor that overshadows them all-the way footwear alters the normal function of the foot.
Symptoms
Plantar fasciitis commonly causes a stabbing pain in the heel of the foot, which is worse during the first few steps of the day after awakening. As you continue to walk on the affected foot, the pain gradually lessens. Usually, only one foot is affected, but it can occur in both feet simultaneously.
Diagnosis
Most cases of plantar fasciitis are diagnosed by a health care provider who listens carefully to your description of symptoms. During an examination of your feet, your health care provider will have to press on the bottom of your feet, the area most likely to be painful in plantar fasciitis. Because the pain of plantar fasciitis has unique characteristics, pain upon rising, improvement after walking for several minutes, pain produced by pressure applied in a specific location on your foot but not with pressure in other areas, your health care provider will probably feel comfortable making the diagnosis based on your symptoms and a physical examination. Your health care provider may suggest that you have an X-ray of your foot to verify that there is no stress fracture causing your pain.
Non Surgical Treatment
To alleviate the stress and pain on the fascia, the person can take shorter steps and avoid walking barefoot. Activities that involve foot impact, such as jogging, should be avoided. The most effective treatments include the use of in-shoe heel and arch cushioning with calf-stretching exercises and night splints that stretch the calf and plantar fascia while the patient sleeps. Prefabricated or custom-made foot orthotics may also alleviate fascial tension and symptoms. Other treatments may include activity modifications, NSAIDs, weight loss in obese patients, cold and ice massage therapy, and occasional corticosteroid injections. However, because corticosteroid injections can predispose to plantar fasciosis, many clinicians limit these injections. For recalcitrant cases, physical therapy, oral corticosteroids, and cast immobilization should be used before surgical intervention is considered. A newer form of treatment for recalcitrant types of plantar fasciosis is extracorporeal pulse activation therapy (EPAT), in which low-frequency pulse waves are delivered locally using a handheld applicator. The pulsed pressure wave is a safe, noninvasive technique that stimulates metabolism and enhances blood circulation, which helps regenerate damaged tissue and accelerate healing. EPAT is being used at major medical centers.

Surgical Treatment
Most studies indicate that 95% of those afflicted with plantar fasciitis are able to relieve their heel pain with nonsurgical treatments. If you are one of the few people whose symptoms don't improve with other treatments, your doctor may recommend plantar fascia release surgery. Plantar fascia release involves cutting part of the plantar fascia ligament in order to release the tension and relieve the inflammation of the ligament. Overall, the success rate of surgical release is 70 to 90 percent in patients with plantar fasciitis. While the success rate is very high following surgery, one should be aware that there is often a prolonged postoperative period of discomfort similar to the discomfort experienced prior to surgery. This pain usually will abate within 2-3 months. One should always be sure to understand all the risks associated with any surgery they are considering.